
A strong surgical manuscript does more than report outcomes. It persuades journal editors that the research is ethical, clinically relevant, statistically sound, and safe enough to enter the scientific record. In surgical publishing, the stakes are higher than many other academic fields because weak evidence can shape decisions in operating rooms, training programs, and hospital systems.
That is why editors often assess risk before peer review even begins.
Many authors believe rejection happens only because results are uninteresting. In reality, numerous surgical papers are declined because they look unreliable, incomplete, exaggerated, or unsafe. Editors are trained to detect warning signs quickly. If those signals appear in the title, abstract, methods, or discussion, the manuscript can be labeled high-risk within minutes.
Understanding these warning signs gives authors a competitive advantage. When you know what editors fear, you can write a paper that feels trustworthy from page one.
Why Surgical Publishing Faces Higher Editorial Scrutiny
A journal article in surgery is not simply an academic exercise. It may influence:
- Procedural choices
- Device adoption
- Postoperative management
- Resident training methods
- Risk counseling for patients
- Hospital protocols
If a flawed paper promotes a poor technique, complications may follow in real clinical environments. Editors know this. That is why they often apply stricter judgment to surgical research than to lower-risk observational topics.
According to the World Health Organization, patient safety remains a global healthcare priority, especially in procedural medicine where preventable harm can occur through systems failure, poor training, or weak evidence. When editors review surgical submissions, they are indirectly protecting patient safety standards.
This is why a manuscript can be rejected even when the writing is polished. If the evidence appears dangerous, weak, or misleading, style will not save it.
Weak Ethics Statements Immediately Damage Trust
One of the fastest ways to make a surgical manuscript look high-risk is poor ethical transparency.
Editors expect clear statements about:
- Institutional Review Board or Ethics Committee approval
- Consent procedures
- Protection of patient identity
- Trial registration where required
- Data handling and confidentiality
- Conflict of interest declarations
When authors vaguely state “ethical approval was obtained” without naming the institution or reference number, concern rises instantly.
Surgery often involves invasive treatment, imaging, tissue samples, device use, or vulnerable patients. Because of this, ethical oversight must be stronger, not weaker.
For example, a retrospective review of laparoscopic outcomes may still require institutional approval depending on jurisdiction. A case report with images usually needs consent. A robotic surgery evaluation involving new technology may need additional governance.
If none of this is clearly explained, editors begin asking a difficult question: If ethics are vague, what else is vague?
Many strong studies fail here because authors underestimate how central ethics is to editorial trust.
Overclaiming Results Makes Editors Skeptical
Some authors try to “sell” their findings too aggressively. This is a major mistake.
A study of 32 patients with short follow-up should not claim to redefine global practice. A single-center audit should not describe itself as definitive evidence. A retrospective comparison should not imply randomized certainty.
Editors are highly sensitive to inflated language because it often masks weak methods.
Common Overstatement Examples
| Study Design | Weak Claim | Better Claim |
| Small case series | New gold standard | Early promising outcomes |
| Single-center review | Proven safest technique | Requires multicenter validation |
| Retrospective cohort | Definitive superiority | Association observed |
| Six-month follow-up | Durable long-term success | Short-term results only |
Strong researchers understand restraint. Honest conclusions often impress editors more than dramatic ones.
When your discussion section sounds like marketing copy, your paper begins to look risky.
Poor Reporting of Surgical Complications Is a Major Red Flag
No operation is complication-free across all patients. Editors know this better than authors sometimes realize.
If your outcomes appear unrealistically perfect, suspicion grows quickly.
That does not mean good outcomes are impossible. It means complication reporting must be transparent, complete, and credible.
A trustworthy paper should clarify:
- Wound infection rates
- Bleeding events
- Anastomotic leaks where relevant
- Readmissions
- Reoperations
- Mortality
- Conversion to open surgery
- Length of stay
- Functional recovery timelines
When authors report only success metrics and omit adverse events, editors may assume selective reporting.
For example, stating that 95% of patients were discharged early is incomplete if 12% required emergency readmission later. Likewise, praising cosmetic outcomes while ignoring nerve injury rates is misleading.
Transparent complication reporting does not weaken a paper. It strengthens it.
Inconsistent Numbers Destroy Confidence
One of the most common reasons editors distrust a manuscript is inconsistent data.
Examples include:
- 148 patients in the abstract, 152 in methods
- Different complication totals across tables
- Follow-up duration changing between sections
- Percentages that do not equal raw numbers
- Missing participants with no explanation
These errors suggest poor quality control.
Even if the science is legitimate, inconsistent reporting creates uncertainty. Editors may wonder whether the database was mishandled, statistics were rushed, or the manuscript was assembled carelessly.
Before submission, authors should manually cross-check every number in:
- Title and abstract
- Main text
- Tables
- Figures
- Supplementary files
In surgery, precision matters clinically and editorially.
Weak Methods Make Strong Results Irrelevant
Many papers report impressive outcomes but fail to explain how the study was conducted.
That is fatal.
Editors need to understand:
- Inclusion and exclusion criteria
- Surgical indication thresholds
- Surgeon experience level
- Technique standardization
- Postoperative protocols
- Follow-up schedule
- Statistical methods
Without this information, readers cannot judge whether results are reproducible.
Imagine a paper claiming low complication rates for a new colorectal approach but never stating whether all operations were done by one expert surgeon or multiple trainees. That missing detail changes interpretation dramatically.
Methods sections are not filler. They are the foundation of credibility.
Language Problems Can Make Good Research Look Unsafe
Many excellent international studies are rejected because the presentation obscures the science.
Editors review high volumes of submissions. If a paper is confusing, they may not invest extra effort to decode it.
Language issues that increase perceived risk include:
- Ambiguous operative descriptions
- Contradictory timelines
- Poor grammar in consent statements
- Unclear endpoint definitions
- Repetitive, bloated discussion sections
- Misused medical terminology
For example, mixing “morbidity,” “complication,” and “adverse outcome” as if they mean the same thing creates confusion.
Clear language signals organized thinking. Chaotic writing signals hidden problems.
This is why professional editing support can materially improve acceptance odds for non-native English-speaking researchers.
Statistical Weakness Is a Silent Rejection Trigger
Editors may not always be statisticians, but they know when numbers look unsafe.
Frequent warning signs include:
- No sample size justification
- Multiple subgroup comparisons with no correction
- P-values without confidence intervals
- No handling plan for missing data
- Misuse of mean instead of median for skewed data
- Claims of equivalence without proper design
A paper may look clinically exciting but still collapse under statistical review.
For example, if two techniques show “no significant difference,” that does not automatically mean they are equally effective. It may simply mean the study was underpowered.
Surgical authors must understand that statistics are not decorative. They determine whether conclusions deserve publication.
Failure to Address Bias Raises Editorial Concern
Every study has limitations. Editors do not reject limitations—they reject denial.
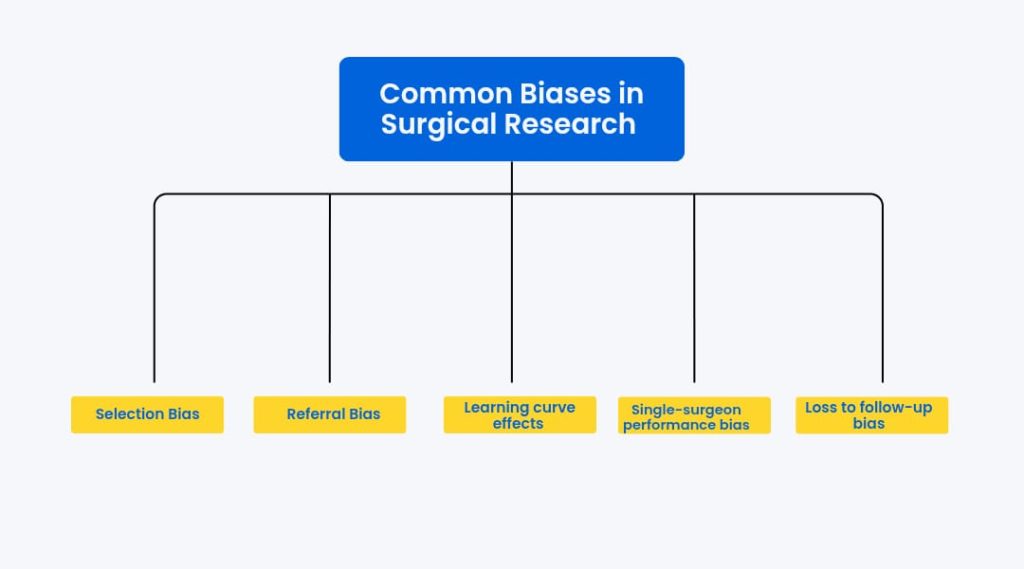
A mature discussion section openly addresses these issues.
For example:
- Were healthier patients chosen for minimally invasive surgery?
- Were complex cases diverted to open procedures?
- Did outcomes improve over time as surgeons gained experience?
If authors ignore obvious sources of bias, editors may view the manuscript as intellectually dishonest.
Irrelevant Keyword Stuffing Looks Amateur
Some authors attempt search-engine thinking inside academic publishing. They insert unrelated terms such as:
- surgical tech jobs
- surgical technologist jobs
- how much does a surgical tech make
- intuitive surgical careers
Unless the study is about workforce economics or staffing trends, these phrases do not belong in a scientific paper.
Likewise, irrelevant stationery-style phrases such as blank manuscript paper or free manuscript paper have no place in clinical scholarship.
Editors notice when keywords feel artificial. It signals poor judgment and weak academic focus.
A manuscript should optimize for discoverability through relevance, not clutter.
Poor Context Around Surgical Training Weakens Education Papers
If your paper discusses residents, simulation, credentialing, or workforce pathways, context matters.
Many authors mention core surgical training without explaining the national system involved. Readers outside that region may not know what it means.
If discussing the UK pathway, clarify:
- Entry stage
- Duration
- Competency structure
- Assessment relevance
When asking what is core surgical training, editors expect precise educational framing, not vague references.
Training manuscripts become high-risk when they assume all readers share local knowledge.
Device and Innovation Papers Face Extra Scrutiny
Studies involving robotics, implants, AI navigation, or novel tools often attract attention—but also suspicion.
Why? Because innovation can be influenced by hype, sponsorship, or early adopter bias.
If your manuscript references systems linked to intuitive surgical careers or commercial ecosystems, editors may closely examine:
- Funding sources
- Author affiliations
- Learning curve effects
- Cost transparency
- Comparative fairness
A paper praising technology without discussing cost, access, or limitations may look promotional rather than scientific.
Innovation papers must work harder to prove neutrality.
What Editors Want Instead of High-Risk Signals
Editors are not searching for reasons to reject. They are searching for reasons to trust.
A low-risk surgical manuscript usually demonstrates:
Clear Ethics
Named approvals, consent details, transparency.
Honest Claims
Conclusions proportional to evidence.
Full Outcome Reporting
Successes and complications both shown.
Strong Methods
Replicable design with logical endpoints.
Clean Statistics
Appropriate tests and clear interpretation.
Balanced Discussion
Limitations openly acknowledged.
Professional Writing
Precise, readable, disciplined language.
These features reduce uncertainty and make peer review smoother.
Practical Checklist Before Submission
Use this final screen before sending your paper:
| Question | If No, Fix It |
| Are ethics approvals explicit? | Yes |
| Do all numbers match? | Yes |
| Are complications fully reported? | Yes |
| Are claims proportional to evidence? | Yes |
| Are limitations acknowledged? | Yes |
| Is language publication-ready? | Yes |
| Are keywords relevant only? | Yes |
If several boxes remain unchecked, editors may classify the submission as high-risk immediately.
Final Thought
Most surgical manuscripts are not rejected because the topic lacks importance. They are rejected because confidence was never established.
Editors protect journals, readers, and ultimately patients. They look for warning signs that suggest bias, weak governance, careless reporting, exaggerated claims, or unsafe interpretation.
The solution is straightforward: write a paper that feels rigorous, transparent, and intellectually honest.
When your surgical manuscript communicates discipline instead of uncertainty, editors notice—and that is where publication momentum begins.
References
- World Health Organization. Patient Safety Overview. https://www.who.int
- International Committee of Medical Journal Editors (ICMJE). Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals. https://www.icmje.org